
Introduction
Rising operational costs are a persistent challenge for privately owned businesses. According to MGMA's 2025 benchmarking analysis, median total operating costs per FTE rose 71.6% from 2011 to 2024 — compared to just 39.5% CPI growth over the same period. That gap represents cost drift: spending that outpaces inflation because no systematic review is catching it.
For smaller, privately owned businesses, rising costs create a specific kind of pressure. Unlike large enterprises with deep reserves, they have less room to absorb margin compression before it affects staffing decisions, capital reinvestment, and long-term viability.
Most operational costs don't become excessive because of market forces alone. Unchecked decisions, outdated processes, and limited strategic oversight are the more common culprits — and the spending behind them was often defensible at some earlier stage. It simply was never revisited.
This article examines where operational costs originate, which drivers most frequently compress margins, and what strategies across procurement, daily operations, and organizational structure can realistically address them.
Key Takeaways
- Operational costs build quietly across labor, supply chain, administrative overhead, and vendor relationships — often invisible until margins force a review.
- Labor consistently represents the single largest cost driver, often exceeding 50–60% of total operating expenditures.
- Effective cost reduction targets root causes — pre-operational decisions, daily management practices, or structural inefficiencies.
- Cutting costs without analysis creates new problems; data-informed strategies produce results that actually hold.
- Outside consulting surfaces cost drivers that internal teams have normalized and stopped questioning.
How Operational Costs Build Up
Cost overruns rarely announce themselves. There's no single line item that explains a margin shortfall. Instead, costs accumulate across dozens of categories simultaneously, compounding until a budget review or financial stress event makes the problem visible.
AHA data from 2024 illustrates how multi-category accumulation works in practice. From 2019 to 2022, labor expense rose 24.7%, supply expense rose 18.5%, and administrative costs trended upward simultaneously.
No single increase triggers a crisis. Together, they do.
The Cost-Drift Problem
For privately owned businesses, the trajectory is especially telling. MGMA's 2025 benchmarking analysis found that median total operating cost per FTE rose 71.6% from 2011 to 2024 — compared to 39.5% CPI growth over the same period. That gap represents cost drift: spending that outpaces inflation because no systematic review is catching it.
The typical triggers for this drift:
- Hiring to meet demand without reviewing the overall staffing model
- Renewing vendor contracts year after year without competitive pricing review
- Absorbing compliance overhead from regulatory changes that was never rationalized afterward
- Paying for software functionality or subscriptions that were partially implemented and never fully adopted
Most of these costs stay hidden until a stress event forces the issue: an audit, a budget shortfall, or an ownership transition. Organizations without a regular operational review process are particularly exposed, because cost accumulation can run undetected for years before it shows up in the margins.
Key Cost Drivers in Business Operations
You can't reduce costs you haven't mapped. Business cost profiles combine fixed structural costs — facilities, equipment, core staff — with variable and semi-variable costs like contract labor, supply utilization, and administrative services. Most reduction opportunities sit in the variable and semi-variable categories, where decisions and oversight have real leverage.
Labor
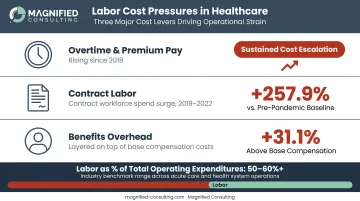
Labor is the dominant cost driver across most business settings. Support staff salaries and benefits can account for a substantial share of total revenue, and total labor — including management and production staff — can consume 50–60% or more of operating expenditures.
Within labor, the specific cost levers that most affect the total are:
- Overtime and premium pay have trended upward since 2018 and are among the most correctable cost problems when caught early
- Contract labor costs rose significantly from 2019 to 2022 — a direct consequence of inadequate permanent staffing plans
- Benefits add roughly 31% on top of base compensation per BLS data, meaning every full-time hire carries substantial cost beyond salary
Supply Chain and Administrative Overhead
Labor dominates the cost profile, but supply chain and administrative costs compound the pressure. Supplies and materials typically represent 5–10% of operating expenses for service-based businesses, with facility costs adding another 5–10%. Those figures seem modest in isolation — without active vendor management, they compound into significant overruns.
Administrative costs are the less visible but no less damaging category. Billing and processing-related costs can represent 10–15% of total professional revenue in service operations. That's a substantial revenue drain before a single service resource is used.
Cost-Reduction Strategies for Business Operations
Effective cost reduction depends on identifying where cost originates — because strategies must match the source. The strategies below are organized by source: decisions that locked in cost trajectories, daily management practices, and the structural environment surrounding the organization.
Strategies That Target Decisions
These strategies focus on reducing cost by revisiting choices that locked in cost trajectories — service offerings, vendor selections, staffing structures, and purchasing defaults.
Apply a sunset review to recurring expenses. Systematically evaluate every non-essential line item by asking what would happen if it were eliminated. Use external benchmarking data to identify spending that exceeds industry norms without proportionate operational value.
Consolidate procurement through competitive bidding or group purchasing arrangements. Rather than defaulting to existing vendor relationships, take the top spending categories and solicit competitive bids. Group purchasing participation, in particular, gives smaller businesses access to pricing leverage typically reserved for large enterprises. Research has found that GPO participation reduces supply-related purchasing costs by 13.1% compared to organizations that source independently.
Revisit staffing structure before filling open roles. Model the full cost of full-time versus part-time for each open position. Benefits add roughly 31% to total compensation for full-time employees. A strategic mix of full-time and part-time staff often reduces benefits overhead without sacrificing coverage capacity.
Convert siloed time-off policies to consolidated PTO structures. This reduces unplanned absenteeism, gives employees more schedule predictability, and typically results in a net reduction in total time-off days granted — a staffing cost implication frequently overlooked in operational reviews.
Strategies That Target Daily Management
These strategies improve cost outcomes through better control, visibility, and consistency in daily operations — not by eliminating resources, but by managing them more precisely.
Monitor labor costs in real time, not retroactively. Overtime is among the most correctable cost problems, but only when identified before it compounds. Organizations that review labor data weekly rather than monthly consistently identify opportunities to realign scheduling before overtime becomes entrenched.
Use operational systems to their full capacity. Platforms and software are only as valuable as how they're used. Organizations that shift document-heavy processes to digital reduce direct supply costs — paper, printing, physical routing — along with the staff time those workflows consume.
Benchmark key expense categories against industry peers on a regular cadence. Cost drift is common when no baseline exists for comparison. Establishing a benchmarking schedule catches anomalies before they become entrenched.
Implement data-driven scheduling aligned to actual demand. Staffing misaligned to volume — overstaffed during slow periods or chronically reliant on last-minute fill-ins — is a direct cost problem. Structured scheduling data can address it without reducing service quality.

Strategies That Target Structural Conditions
Some cost problems aren't rooted in how an organization runs day to day — they're baked into the physical footprint, contract structures, and structural conditions the organization operates within. These strategies address that layer.
Restructure physical space utilization. Administrative square footage that generates no revenue represents a fixed cost that can be converted. Consolidating workspaces and repurposing freed space into revenue-generating areas can meaningfully reduce fixed cost exposure.
Align cost structures with revenue realities. Organizations still operating under volume-based assumptions may be absorbing costs that current service models don't compensate. Mapping cost structures against actual revenue streams — with consultant support — identifies where spending exceeds what the operating model rewards.
Engage outside advisory support for the cost drivers internal teams can't see. One of the most consistent findings in operational consulting is that significant inefficiencies are often absorbed over time by the people closest to them. External advisors bring the objectivity and cross-organizational benchmarking to surface those blind spots. Firms like Magnified Consulting work with privately owned and family-run businesses to surface those gaps — bringing a structured analytical framework and cross-industry benchmarking perspective that internal teams, regardless of capability, rarely have the distance to apply on their own operations.
Conclusion
Reducing operational costs requires knowing where cost originates — in decisions, in management practices, or in structural conditions. Across-the-board cuts that address symptoms without resolving root causes tend to create new problems while leaving the underlying cost trajectory intact.
Sustainable cost reduction is a continuous discipline, not a one-time project. Organizations that embed it into their operating model — through regular benchmarking, structured reviews, and outside advisors who bring data and objectivity — protect margins without sacrificing the capacity to grow. That combination is what separates businesses that weather financial pressure from those that get caught reacting to it.
Frequently Asked Questions
What are cost reduction strategies in business operations?
Business cost reduction strategies span three areas: procurement (vendor negotiation, competitive bidding, eliminating non-essential services), operational management (labor scheduling, system utilization, benchmarking), and structural changes (space optimization, operating model alignment). Effective strategies target identified cost drivers rather than applying cuts uniformly across the organization.
How can businesses reduce operational costs?
The primary levers are controlling labor costs through better scheduling and reduced overtime reliance, renegotiating supply and vendor contracts, maximizing existing technology investments, and engaging outside consultants for objective operational assessments. The best results consistently come from addressing multiple cost categories simultaneously rather than isolating a single fix.
What is the biggest operational cost in a business?
Labor is consistently the largest single operational cost, often exceeding half of total operating expenses. The highest-impact factors within labor are overtime, premium pay rates, contract staff dependency, and benefits overhead — which can add roughly 31% to base compensation costs.
How do business consultants help reduce costs?
Experienced consultants focus first on administrative, procurement, and structural inefficiencies — areas that don't directly touch core service delivery. Optimizing these functions reduces costs while preserving the resources available for client-facing operations.
How long does it take to see results from cost reduction efforts?
Procurement changes and scheduling adjustments can show measurable impact within weeks, while structural and operational redesigns typically take three to six months. Organizations working with structured consulting frameworks tend to move faster, since root causes are identified early rather than uncovered late in the process.
What areas should businesses prioritize when cutting costs?
Start with areas that are both high in spend and high in controllability: labor scheduling and overtime management, vendor contracts in the top 20% of spend categories, and underutilized technology. Once those are addressed, structural changes — space optimization, operating model alignment — require more planning but typically produce the most durable long-term savings.


